Overview
The skin is a complex active organ, if any of its functions fail there can be serious consequences. The skin's ability to act as a barrier is particularly important for occupational health.
One way to understand the barrier function of the stratum corneum is to consider it as a brick wall. The corneocytes (made of tough protein) form the bricks and between these a double layer of lipids (fatty materials) and water make up the mortar. Some lipids have a hard crystal-like structure and are impermeable to water. Others lipids do not have this structure and they allow water to percolate through. So, the barrier is semi-permeable.

The elasticity, firmness and correct functioning of the stratum corneum depends on its moisture content. Retention of water is aided by substances in the skin called natural moisturising factors (NMFs). If the moisture content is too high or too low, it can affect the skin's barrier properties.
If the skin becomes overhydrated, for example from prolonged contact with water or from wearing gloves that prevent sweat from evaporating, it causes NMF production to stop.
If the skin dehydrates, for example in an air-conditioned environment with low humidity, the corneocytes are not shed as normal and the skin becomes rough, thickened and flaky, eventually leading to cracking because of loss of elasticity.
The 'surface film' on the epidermis also acts as a barrier, to prevent bacteria and other contaminants from penetrating the skin. The film is slightly acidic and can help to neutralise the contaminants that are typically alkaline in nature. Excessive use of harsh alkaline soaps can destroy the acidity of the film and hence the protection it offers.
Problems occur when the skin's barrier is breached. This can happen when:
- a material/agent penetrates the barrier layer or alters it so other materials/agents can penetrate it;
- a material/agent enters sweat ducts or hair follicles, by-passing the barrier layer.
How does the skin react to 'breaches'?
The skin has a limited range of protective responses. The most common one is inflammation. This is known as dermatitis or eczema. It is characterised by redness and heat from dilation of local blood vessels, swelling and blistering from plasma leaking from the vessels to the surrounding tissue and itch caused by stimulation of nerve fibres. Secondary changes due to infection and scratching include crusting, ulcers and thickening of the skin.



Dermatitis caused by a malfunction or disorder within the body is termed endogenous or constitutional dermatitis. Work-related dermatitis is due to contact with some external agent. This is known as exogenous dermatitis or more commonly contact dermatitis.
External agents tend mostly to come into contact with the hands and forearms, so around 95% of work-related skin diseases occur in this area. The majority of the remainder are on the face. Most work-related skin diseases are contact dermatitis. External agents are involved in an important minority of other work-related skin diseases. These include contact urticaria, acnes, cancers, leucoderma (vitiligo) and skin infections.
Contact dermatitis
Identifying 'abnormal' skin can be straightforward but identifying the cause is more complex. It is helpful for health and safety and medical professionals to work together to establish whether the condition is work related.
The majority of work-related skin diseases are dermatitis. So, the first step is to establish whether the skin problem is dermatitis. This can be quite challenging for medical professionals since the appearance of both acute and chronic dermatitis can vary and it can be presented to the doctor at different stages. Also, there are some common skin conditions, which are confused with dermatitis: psoriasis, pustulosis of the palms and soles, tinea, scabies, lichen planus.
If the condition is dermatitis, the next question is whether it is constitutional or if it arises from contact with an external agent, ie contact dermatitis. An important clue is the site of the area affected. If it is the hands, contact dermatitis should always be suspected.
The final question is whether the 'contact' arises from work or from home. Medical practitioners will take a range of factors into consideration when making a diagnosis, including the site and spread of rash, history of onset, work done by the patient, hobbies and medications.
Some helpful clues to recognise a work-related cause are:
- if it is primarily on the hands and face;
- if the condition improves away from work and relapses on return;
- if more than one person affected in same work area or handling same materials.
There are two main types of work-related contact dermatitis, irritant contact dermatitis and allergic contact dermatitis.
Irritant contact dermatitis
An irritant directly damages cells if in contact with the skin in sufficient concentration and for sufficient time. Most irritants cause dermatitis by gradually overwhelming the skin's barrier and repair mechanisms. Mild irritants such as detergents will wash out the stratum corneum lipids and if exposure exceeds the capacity of the skin to regenerate those lipids, dermatitis will result. Powerful irritants ‑ such as caustic soda ‑ produce an immediate effect. These cause direct damage to keratinocytes. Dermatitis induced by mild irritants is called chronic or cumulative irritant contact dermatitis.
People vary in their susceptibility to irritants. For reasons not yet understood, certain groups of people are more susceptible to irritants:
- those with constitutional dermatitis/eczema (known as 'atopics');
- those with very dry skins;
In general, irritant contact dermatitis is more common occupationally than allergic contact dermatitis. There are a number of occupations and materials associated with irritant contact dermatitis. It is important to realise that contamination of the skin from a 'dirty job' rarely causes irritant dermatitis, it is more commonly the cleansers used to remove the contamination. The effect is exacerbated in winter by environmental factors (wind, cold) which cause drying of the skin. It is not unusual to see more cases of hand dermatitis in the winter and it is particularly important for employees at risk to know how to protect themselves during the winter months.
Allergic contact dermatitis
Allergic contact dermatitis is caused by contact with a 'sensitiser' (allergen) that causes a type IV or 'delayed hypersensitivity' reaction. A sensitiser is a substance that can induce an 'over-reaction' of the body's immune system.
A sensitiser must first penetrate the skin (most contact sensitisers are small molecules with molecular weights below 1000). Next the sensitiser is combined with skin immune cells (Langerhans cells) which then leave the skin and travel to lymph glands nearby (known as induction). Here, they react with another type of immune cell (T-lymphocytes or T-cells), which reproduce and produce 'memory' cells that can remember that particular sensitiser.

Once sensitisation has occurred, subsequent contact causes T-cells to recognise the sensitiser and multiply. This induces the release of substances such as histamine that bring about the features of inflammation (known as elicitation). This second phase can happen hours or days following contact hence its name 'delayed hypersensitivity'. Very small quantities of the sensitiser can trigger a response once sensitised.
There is a range in potency for sensitisers. The initiation of sensitisation may occur at the very first contact or it may not happen until there has been repeated contact for months or even years. The process of sensitisation produces no visible change in the skin.
Generally, only a small proportion of an exposed occupational group becomes sensitised. It depends on the concentration of sensitiser and the degree and duration of skin contact ‑ as well as the sensitising potential of the sensitiser.
Sensitisation is specific to one substance or to a group of substances that are chemically similar. Once sensitised a person is likely to remain so for life.
Both irritant and allergic contact dermatitis can occur together (particularly on the hands) and either may co‑exist with constitutional dermatitis. It is common for exposure to occur to more than one irritant and more than one allergen at any one time. Such exposures may give rise to a cumulative irritant and cumulative allergic response. An irritant contact dermatitis may also develop first, rendering the skin more susceptible to penetration by sensitisers. It is also possible that an original allergic contact dermatitis might be later sustained by an irritant.
There are a number of occupations and materials associated with allergic contact dermatitis. Some substances can act both as irritants and sensitisers, for example cement; its wetness, alkalinity, grittiness and hygroscopicity make it an irritant. It contains the sensitisers chromate and cobalt.
Contact urticaria
Contact urticaria is a wheal-and-flare (small swellings on the skin surrounded by areas of redness) response occurring rapidly on the application of certain substances to intact skin. It is probably more common than currently recognised. It can arise from different mechanisms:
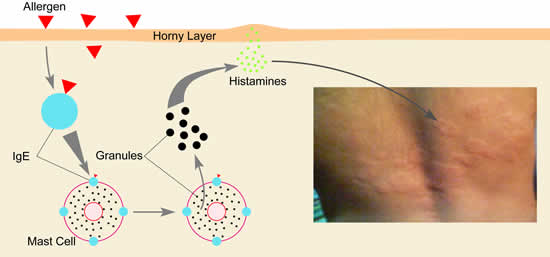
- An immunological mechanism. Like allergic contact dermatitis, it depends on previous exposure to the substance and development of an immune reaction to it, ie sensitisation. The immune cells involved with contact urticaria are called immunoglobulin E or IgE cells. Once sensitised, subsequent exposure causes a reaction between the sensitiser, IgE cells and Mast cells, leading to the release of chemicals that cause an immediate wheal-and-flare response( this is a type I or immediate hypersensitivity response).
- A non-immunological response (direct histamine release). Not all cases are due to sensitisation. The chemicals causing the wheal-and-flare response can also be released by non-allergic mechanisms.
- A large sub-group have unknown causes.
Type I immunological reaction mechanism
Currently, the most important cause of occupational immunological contact urticaria is natural rubber latex. Substances capable of causing non-immunological contact urticaria that are seen occupationally include cobalt and platinum salts and balsams.
Persulphates can cause contact urticaria of uncertain cause in hairdressers and chemical workers.
Common work-related causes can be found in causative agents and occupations at risk.
Acnes
The hair (or sebaceous) follicle is the target organ in both oil acne (or folliculitis) and chloracne, although the two should not be confused.
- Oil acne is the result of irritation of the hair follicle by residues of mineral oil remaining on the skin as the result of poor hygiene. It tends to occur under oil-soaked working clothing on the forearms and thighs of machine tool operatives.
- Chloracne is a far more specific effect of certain poly-halogenated aromatic hydrocarbons, such as the chlorodibenzodioxins, on the sebaceous follicle. It can be a comparatively mild condition, confined to the face and neck, though severe cases also occur. There may only be small groups of open comedones (blackheads) in the cheek areas and one or two characteristic 'blind' straw-coloured cysts behind the ears.
The importance of detecting such minor occupational cases is the possibility of systemic toxicity from chloracnegens (causative agents). At present, evidence suggests that the external dose of a chloracnegen required to cause chloracne is significantly lower than that needed to cause systemic disorders (changes in circulating blood lipid levels, porphyria or any form of neoplasia/tumour).
Cancers
Workplace skin contact with certain materials can lead to skin cancer and some materials will readily penetrate the skin and cause cancers elsewhere in the body. There are a range of materials associated with skin cancer.
Squamous cell cancer, cancer arising on the external surface of the skin, can be caused by the following:
- polycyclic aromatic hydrocarbon compounds (PAHs) from chronic exposure to coal tar products and mineral or shale oils;
- unrefined mineral oils causing scrotal skin cancer, which should be regarded as occupational until proved otherwise, since the non-occupational disease is extremely rare;
- sunlight and pitch exposures can act synergistically to cause the cancer in occupations such as the removal of pitch based roofing or surface materials;
- sunlight alone may be regarded as an occupational cause in outdoor work such as farming;
- chronic exposure to inorganic arsenic, for example among miners and smelters of arsenical ores, can result in cancers associated with 'raindrop' pigmentation and keratoses (precancerous lesions of the skin).
Basal cell cancers may be caused by skin damage from the sun and are commonly seen in outdoor workers.
Leucoderma (vitiligo)
Melanocytes (pigment-producing cells) can be selectively destroyed by certain workplace chemicals. Paler or completely white patches of skin result (leucoderma/vitiligo). Most cases in the general population are of unknown cause. Around one percent of adults suffer from it. Several cases of leucoderma in one factory should arouse suspicion that there may be a work-related cause.
Some chemicals reported to have had this effect occupationally are:
- alkyl catechols;
- quinones;
- alkyl phenols.
Cases have been described in many occupational groups including chemical workers, engineering workers (from oil), automobile workers (from adhesive) and even hospital personnel (from germicide).
Skin infections, infestations and insect bites
Skin infections, infestations and insect bites may be occupational in origin:
- bacteria (eg impetigo);
- viruses (eg orf);
- fungi (eg tinea pedis in miners);
- yeasts (eg candidal paronychia in wet workers);
- arthropods (eg 'grain itch' from mites);
- Protozoa (eg Leishmaniasis).